

A great deal of last week’s Democratic debates centered on healthcare.
And when the chilling words “Medicare-for-All” are spoken, there is inevitably someone–moderate Democrat or Republican–who is going to turn around and trot out right-wing talking points about “doctors leaving Canada for the United States,” and Canadian patients with serious health issues having to languish on interminable waiting lists.
Naturally, we want a president bold and progressive enough to take on the for-profit health insurance industry that has exploited millions of Americans’ suffering to make a handful of CEOs and politicians fabulously wealthy.
First, let me state I am not Canadian.
I went to Canada once the summer before ninth grade when my family crossed over to the Canadian side of Niagara Falls.
I’ve met Canadians, and have researched their healthcare system and what they think about it.
Many have gone public pointing out the inaccuracies our corporate media deftly promulgates.
Canada is not some third-world banana republic where people are dying in the streets. It’s a civilized liberal Democracy, as is Denmark, Germany, New Zealand, Sweden, Switzerland, Great Britain, Finland, Japan–all countries with some form of national healthcare service.
And they are proud and fiercely protective of their national healthcare system.
Most countries offer healthcare as a human right to all its citizens.
But of the 25 wealthiest nations, the United States is the only one that fails to do this.
As an American with decent employer-provided private health insurance who has received letters explaining how doctor-prescribed medical procedures are being declined because they have been deemed “unnecessary,” I know there is something fundamentally flawed with the ways in which we deliver healthcare in America.
I acknowledge my good fortune.
My wife, children, and I are healthy. Our co-payments are reasonable, and we have not ever hit the insurance provider’s arbitrary cap.
Yet I also acknowledge millions of our fellow countrymen are not as fortunate. They have high deductibles, co-payments, may have lousy coverage, and are one serious illness or injury away from bankruptcy.
Although healthy, my wife, children, and I are going to get sick at some point, hopefully not seriously–but that is always a possibility. We don’t plan for disease, accidents, or medical procedures. My wife had a skin cancer scare a few months back, for example. My son broke his wrist at school in May.
The United States needs a single-payer universal healthcare system because health should not be profitable. Wealthy business leaders, pharmaceutical executives, and politicians who legislate for them should not get rich off others’ pain and suffering.
So since so many of our fellow Americans like to shut down conversations about universal healthcare with Canadian “failures,” let’s drill down a little deeper.
There are many permutations of national healthcare systems, and we do not need to follow Canada–or any other country’s–model in lock step.
Great Britain, for example, practices socialized medicine, in which the government owns and operates most of the healthcare providers and doctors are government employees. Although technically a single-payer system, it is just one model.
Canada and many other nations, on the other hand, contract with private providers in which doctors still run their own practices.
This is the difference between “socialized medicine” and “single-payer.”
Canadian physician Danielle Martin, vice president of medical affairs and health system solutions at the Women’s College Hospital in Toronto, explains:
“The services are paid for through general taxation, but the services are not delivered by government employees. [As] a family doctor, I am not an employee of the government. I deliver my services in a very similarly looking model to American physicians. But instead of billing a private insurance company or billing my patients directly, I simply bill the government plan.”
There is not a single Democrat advocating turning the medical profession over to Washington. The Medicare-for-All single-payer system Senator Bernie Sanders is proposing, for example, would merely require the government to foot the bills. Doctors would still be in charge of providing care, and they and only they would be making the decisions, not wealthy executives in suits or call center customer service representatives reading from scripts.
“Wouldn’t this create a complete bureaucratic mess?” someone is bound to ask. “Never trust the government!”
While it’s probably prudent to maintain a healthy skepticism about what our government is or is not up to, consider that the for-profit insurance industry is cited as one of the most bureaucratic in the world. Roughly around 30% of every dollar spent on healthcare in America is put toward paperwork, salaries, and administrative overhead. Canada, by comparison, boasts only one percent. Our Medicare program–passed 50 years ago–boasts two percent.
Remember, the private health insurance industry’s goal–as is any industry’s–is to maximize profit. This is not the government’s objective.
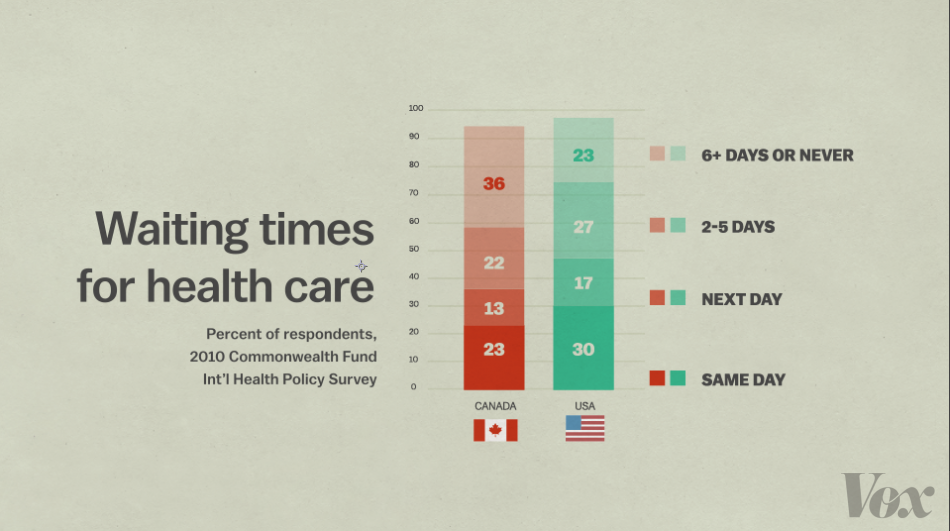
But what about the “fact” people are dying in Canada because they have to wait so long for care?
The fact is, they aren’t.
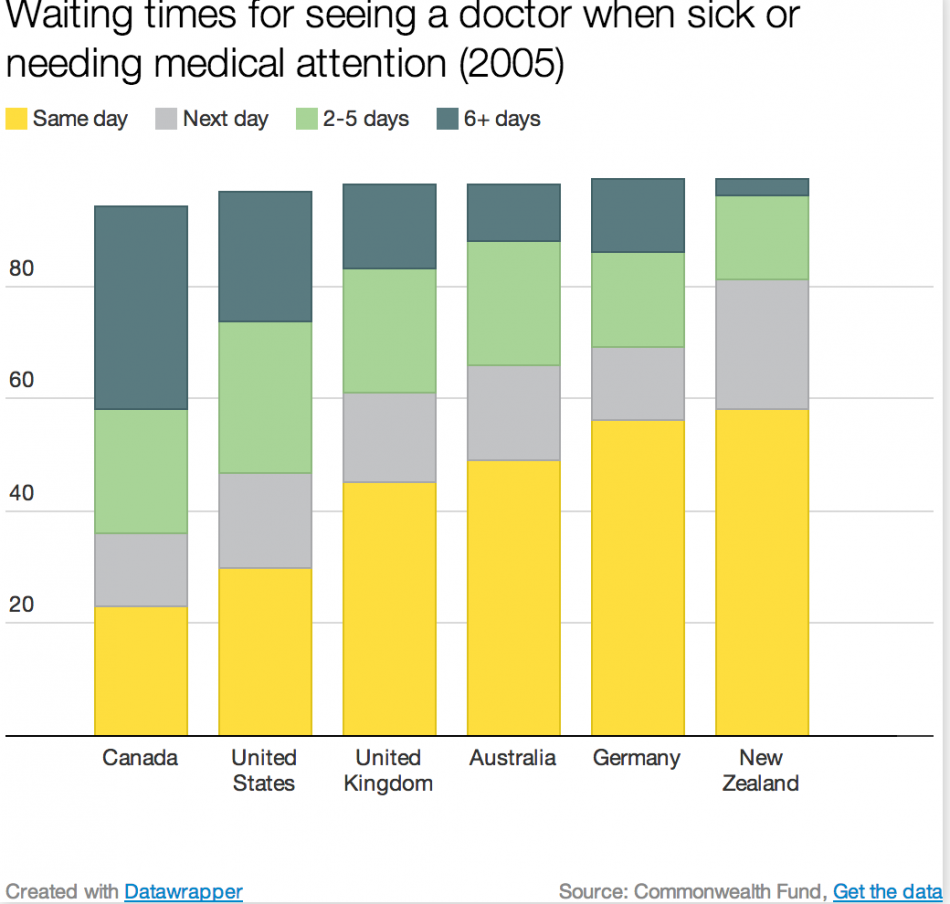
There are no waits for urgent or primary care in Canada.
As is the case here, there are reasonable wait times for specialists. What many either fail to realize or conveniently omit is that wait times are longest for elective surgery.
Dr. Danielle Martin explains:
“I think it’s critical for people to know that when Canadians are seriously sick—when the issue is urgent—they don’t wait. So this myth that people are sort of dying in the streets, waiting for care is just that—a myth. Part of the reason that we know that is because our health outcomes are good. When compared to the U.S., outcomes for a whole variety of different diagnoses—including life expectancy, including infant mortality—all of these things actually, the Canadian system delivers as good or better care on average across the population than we see in the U.S.”
According to the U.S. Cancer Statistics Working Group and the Canadian Cancer Society, Canadians experience lower incident and mortality rates than we do for all cancers combined.
10 years ago, 11.3 percent of Canadians reported unfulfilled healthcare needs compared to 14.4 percent here.
To claim we don’t wait for specialists is naive.
Anyone who has had to schedule an appointment lately knows there is a specialist for everything in America, and getting in to see him or her is frustrating and cumbersome. Just making an appointment with primary care physicians can involve unreasonable waits. This is due to a paucity of physicians. We need more doctors.
So does Canada. For all its benefits, healthcare in the southern region of the country, where the major cities are located, have shorter wait times because there are more doctors. Rural areas further north have fewer, increasing wait times.
The situation is similar here.
Another claim floating around out there is that Canadians pay WAY TOO MUCH in taxes and their healthcare is too expensive.
Also not true.
Dr. Danielle Martin explains:
“The United States pays more per capita for health care than any other country in the world. You’re closing in on 20 percent of your GDP in terms of what you spend. We in Canada spend 10 percent of our GDP on health care services and we cover virtually every single resident of our land. That’s what I think is the more important question…not how much you pay via taxes, but how much you pay via taxes, plus out-of-pocket, plus for private insurance, and who’s in and who’s left out, and who’s at risk of not having coverage when they need it most. The last thing you need when you’re sick is to be worried on top of your illness, about how you are going to pay for your care.”
Healthcare costs are the leading cause of bankruptcy in the United States.
We pay a lot in taxes in this country (unless you’re super-wealthy). Consider all the additional costs we incur in prescription drugs and doctor visit co-payments. For too many, it’s too much.
Another complaint about our neighbors to the north is that the government chooses residents’ doctors.
Again, false.
As stated before, Canada contracts with private providers who still run their own practices. Canadians are free to select their doctors, as we are here.
What about the “rationed healthcare” argument we frequently hear from the right?
This was common in 2009-10 when the Affordable Care Act (ACA) was making its way through Congress.
Canada does not “ration” care.
According to the article “10 Myths About Canadian Health Care, Busted” published on the Physicians for a National Healthcare Program (PNHP) website:
“One of the things that constantly amazes me here is how well-cared-for the elderly and disabled you see on the streets here are. No, these people are not being thrown out on the curb. In fact, they live longer, healthier, and more productive lives because they’re getting a constant level of care that ensures small things get treated before they become big problems.
“The health care system also makes it easier on their caregiving adult children, who have more time to look in on Mom and take her on outings because they aren’t working 60-hour weeks trying to hold onto a job that gives them insurance.”
Another gem is when people play the “personal responsibility” card. This is the Libertarian argument that claims people will not have a vested interest in their own health if they are not personally paying for it out of their own pockets.
This is just a fallacy on so many levels, and false.
Even people who eat well, exercise regularly, and mind their weight get sick.
The idea we should not be invested in our fellow countrymen’s health is not only cruel; it’s also bad policy.
If someone gets sick, that person runs the risk of getting others around him or her sick as well. That’s why many employers offer sick days. In theory, if we are ill, we shouldn’t expose our co-workers (or subway and train passengers, or fellow Starbucks patrons) to our illnesses, especially if what we have is potentially worse than the common cold.
Just look what happened this spring when the measles came to New York: the New York Assembly voted to eliminate a vaccine religious exemption for schoolchildren.
This is a prime example of how governments play a vital role in ensuring public health.
Of course, there is the issue of low-wage workers coming to work sick because they don’t have paid sick days. There is no federal law requiring paid sick time, and staying home for themselves, their children, or elderly parents who may be ill could result in someone’s loss of pay.
There is also the productivity loss argument the corporate milieu can appreciate.
When employees are ill, absenteeism affects businesses’ bottom line; when employees report to work sick, they aren’t typically as productive.
Universal healthcare eliminates that burden.
Just think of what happens when an uninsured person reports to the emergency room, which is not legally permitted to turn patients away: everyone else with private insurance pays for it.
If everyone were covered, however, this would not be the case.
This was the reasoning behind the ACA’s individual mandate by requiring everyone to have some form of health insurance coverage, either via an employer or the ACA marketplace.
The Trump administration has effectively destroyed this under a provision in the 2017 GOP tax scam.
Public health in Canada and other nations that practice universal healthcare systems is a duty to the entire society.
But what about the fact that medicine is known to be a very lucrative profession in America? Aren’t doctors under a universal healthcare model not paid as well as they are here?
There are many places to go with this.
There’s the wage argument that states if more people were paid salaries commensurate to their jobs, education, and experience, there would be less income inequality. Raising the minimum wage would address this, as would instituting a universal basic income, as presidential candidate Andrew Yang is proposing.
From a universal healthcare perspective, using Canada as a template, quoting again from the (PNHP) website:
“They [Canadian doctors] don’t have to charge higher fees to cover the salary of a full-time staffer to deal with over a hundred different insurers, all of whom are bent on denying care whenever possible. In fact, most Canadian doctors get by quite nicely with just one assistant, who cheerfully handles the phones, mail, scheduling, patient reception, stocking, filing, and billing all by herself in the course of a standard workday.
“Second, they don’t have to spend several hours every day on the phone cajoling insurance company bean counters into doing the right thing by their patients. My doctor in California worked a 70-hour week: 35 hours seeing patients, and another 35 hours on the phone arguing with insurance companies. My Canadian doctor, on the other hand, works a 35-hour week, period. She files her invoices online, and the vast majority are simply paid—quietly, quickly, and without hassle. There is no runaround. There are no fights. Appointments aren’t interrupted by vexing phone calls. Care is seldom denied (because everybody knows the rules). She gets her checks on time, sees her patients on schedule, takes Thursdays off, and gets home in time for dinner.
“One unsurprising side effect of all this is that the doctors I see here are, to a person, more focused, more relaxed, more generous with their time, more up-to-date in their specialties, and overall much less distracted from the real work of doctoring. You don’t realize how much stress the American doctor-insurer fights put on the day-to-day quality of care until you see doctors who don’t operate under that stress, because they never have to fight those battles at all. Amazingly: they seem to enjoy their jobs.
“Third: The average American medical student graduates $140,000 in hock. The average Canadian doctor’s debt is roughly half that.
“Finally, Canadian doctors pay lower malpractice insurance fees. When paying for health care constitutes one of a family’s major expenses, expectations tend to run very high. A doctor’s mistake not only damages the body; it may very well throw a middle-class family permanently into the ranks of the working poor, and render the victim uninsurable for life. With so much at stake, it’s no wonder people are quick to rush to court for redress.”
Another right-wing talking point we hear frequently is that Canadians are flocking south to see American doctors.
Just think how Fox so-called News would react if this were true. Programming would be simple. All crews would have to do is park themselves outside doctors’ offices waiting for Candian citizens to come out and rave about how great their care was here in the good old U-S-of A.
Donald Trump prates ad nauseum about “migrant caravans” flooding over our Southern border.
If Canadian healthcare were so egregious, wouldn’t there be “caravans” coming from up there as well?
Don’t hear about them, though, do we?
It’s because there aren’t any.
Authors of the study “Phantoms in the Snow: Canadians’ Use of Health Care Services in the United States,” featured in the peer-reviewed journal Health Affairs, surveyed 136 ambulatory care facilities near the Canada border in Michigan, New York, and Washington, and found around 80 percent saw an average of fewer than one Canadian per month; about 40 percent had seen none the prior year.
Looking at the number of Canadians discharged from acute-care hospitals in the same states over a five-year period, researchers found more than 80 percent of hospital visits were for emergency or urgent care, many for tourists. Only about 20 percent were for elective procedures or care.
As Dr. Aaron E. Carroll states in “5 Myths About Canadian Health Care” published on the American Association of Retired Persons (AARP) website:
Surveying America’s 20 “best” hospitals, only one of the 11 respondent hospitals saw more than 60 Canadians a year, including for both emergencies and elective care.
Finally, data from 18,000 Canadians who participated in the survey and had received care in the United States find only 20 reported crossing into the United States expressly to obtain care.
But what about the Canadian doctors leaving Canada to practice in the U.S.?
The Canadian Institute for Health Information has been tracking doctors’ destinations since 1992.
In 2003, 169 physicians emigrated to the States; in 2004, 138; in 2005 and 06, 122—less than 0.5 percent of all Canadian doctors.
In fact, in 2004, more physicians emigrated from the United States to Canada than immigrated to the U.S.
To sum up, we turn to the medical journal The Lancet:
“Access to health care based on need rather than ability to pay was the founding principle of the Canadian health-care system. Medicare was born in one province in 1947. It spread across the country through federal cost sharing, and eventually was harmonised through standards in a federal law, the Canada Health Act of 1984. The health-care system is less a true national system than a decentralised collection of provincial and territorial insurance plans covering a narrow basket of services, which are free at the point of care.”
So the next time you find yourself in a conversation with someone who insists on “proving” to you Canadian healthcare is a failure, show him or her this article.
It may not change his or her mind, but it may shut him or her up.
Image credit: www.writeopinions.com
